Basic Information
Welcome to the Psoriatic Arthritis Symptom Assessor.
The following series of questions will ask about your condition, medical history, and the medications you are taking. At the conclusion of this process, you will be provided a PDF file to download and print that you can bring to your rheumatologist or physician at your next visit.
-
Date of Birth
-
Gender
-
Region
-
Year you were diagnosed with PsA
Would you like to create an account?
If you would like us to remember your answers, please create an account. This will make it a lot faster to complete future assessments.
Account Login
Please login to your account. Forgot your password?
-
E-mail
-
Password
Create New Account
Input your e-mail and password to create an account that will save your history.
-
E-mail Address
-
Password
-
Repeat Password
Your personal information will be kept confidential. Please see our privacy policy.
DMARDs
Please click on any medications that you are taking on the list below.
Biologics
Please click on any medications that you are taking on the list below.
Corticosteroids
Please click on any medications that you are taking on the list below.
NSAIDs
Please click on any medications that you are taking on the list below.
Please provide your medication dosages
For the following medications, please provide your dosage information and how frequent you take it.
Additional Information
Please answer the following additional questions for Hydroxychloroquine (Plaquenil).
-
Are you having your eyes examined at least once per year?
Additional Information
Please answer the following additional questions for Prednisone:
-
When did you have your last bone density test?
-
Are you taking vitamin D?
-
Are you taking Calcium?
-
Please select any bone hardening medications that you are taking on the following list:
Are you using any other medications?
Have you been using any other medications than those listed?
For each other medication, please list: medication + dosage + how often
Experiencing any new problems with your medications?
Have you been experiencing any new problems with your medications since your last visit? If you are not entirely sure then choose yes, you will be asked to provide further details.
Health Changes Since Last Visit
Since the last time you visited your rheumatologist, have you...
-
Had any infections?
-
Had any fevers?
-
Been prescribed antibiotics?
-
When was your last blood test?
Any major health changes since your last visit?
Examples of major health changes can include: being sick or diagnosed with a new disease, having surgery, and any health issues requiring a hospital visit.
Any major life changes since your last visit?
Examples include highly stressful or emotional situations such as: the death of a family member, friend, or pet; job loss; major career changes; or even a big move.
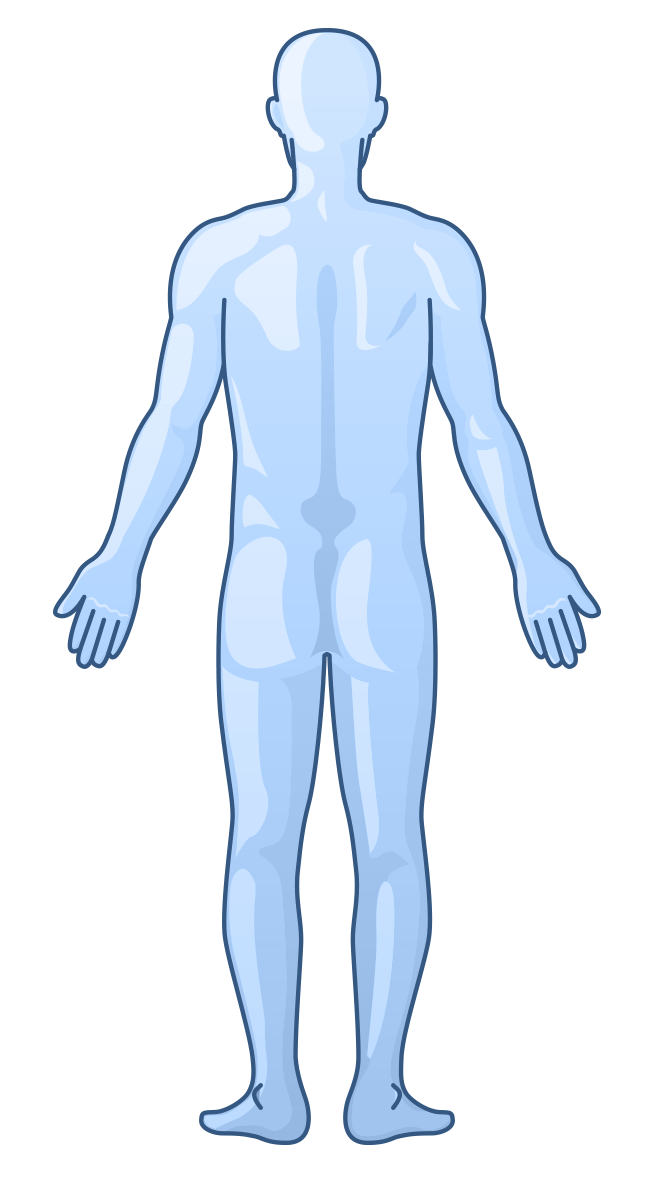
Upper Torso & Arms (Front Facing)
Click where you are experiencing pain or swelling in the diagram below.
Legs (Front Facing)
Click where you are experiencing pain or swelling in the diagram below.
Upper Torso & Arms (Backside)
Click where you are experiencing pain or swelling in the diagram below.
Legs (Backside)
Click where you are experiencing pain or swelling in the diagram below.
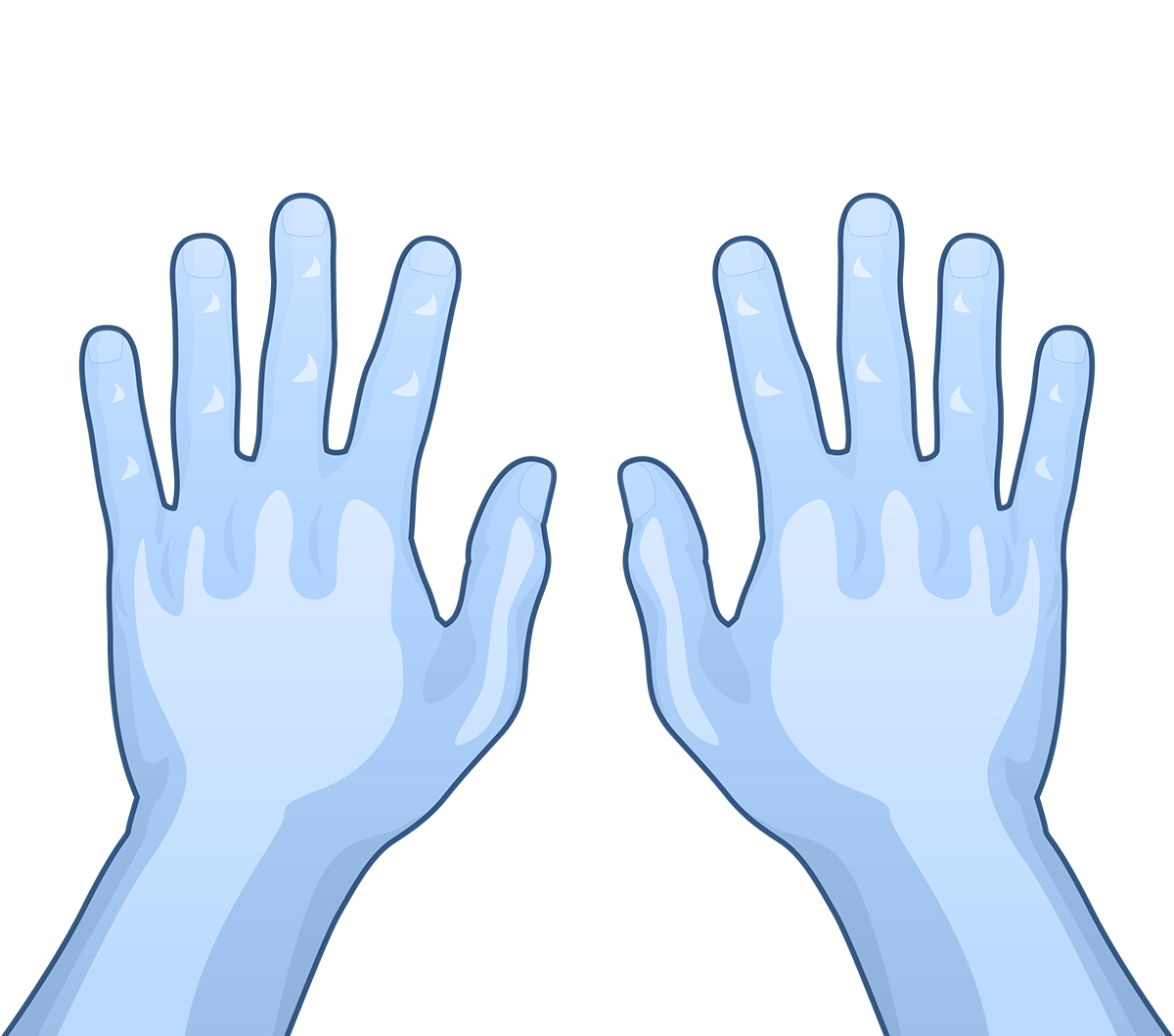
Hands
Click where you are experiencing pain or swelling in the diagram below.
Feet
Click where you are experiencing pain or swelling in the diagram below.
Disability Rating Scales
We are interested in learning how your illness affects your ability to function in daily life. For each of the following questions, indicate which answer best describes your usual abilities over the past week.
How well are you able to:
-
Get on and off the toilet?
-
Open car doors?
-
Stand up from a straight chair?
-
Walk outdoors on flat ground?
-
Wait in a line for 15 minutes?
-
Reach and get down a 5-pound object (such as a bag of sugar) from just above your head?
-
Go up 2 or more flights of stairs?
-
Do outside work (such as yard work)?
-
Lift heavy objects?
-
Move heavy objects?
Activity Scales
Please answer the following questions as related to your arthritis:
-
For how many hours does your morning stiffness last from the time you wake up?
-
How much pain have you had because of your illness in the past week? How much pain have you had because of your illness in the past week?
-
How much of a problem has unusual fatigue or tiredness been for you over the past week? How much of a problem has unusual fatigue or tiredness been for you over the past week?
-
How much of a problem has sleeping been for you over the past week? How much of a problem has sleeping been for you over the past week?
-
Considering all the ways your arthritis affects your life, rate how you are doing on the following scale: Considering all the ways your arthritis affects your life, rate how you are doing on the following scale:
Psoriasis Scales
Please answer the following questions as related to your psoriasis:
-
Considering all of the ways your psoriasis affects your skin, how much of a problem has your skin been over the past week? Considering all of the ways your psoriasis affects your skin, how much of a problem has your skin been over the past week?
-
Considering all of the ways your psoriasis affects your nails, how much of a problem have your nails been over the past week? Considering all of the ways your psoriasis affects your nails, how much of a problem have your nails been over the past week?
Positive Changes
What has changed for the better since you started treatment?
Are you able to do things you couldn't do before, or have less pain?
?>
Discuss With Doctor
Is there anything that you would you like to discuss with your doctor at your next appointment?
Your assessment is Complete!








Your answers will be very helpful to your doctor on your next visit. Please bring the following PDF document to your next appointment.
Download PDF